

Background: Obesity is increasing worldwide, with the highest prevalence in the United States. High or low body mass index (BMI) is a well-established risk factor for increased all-cause mortality and also has been associated with cancer-specific mortality. However, the impact of BMI on survival following diagnosis with lymphoma currently remains controversial. We leveraged a prospective cohort of lymphoma patients to assess the relationship of BMI two years prior to diagnosis (BMI-2), at diagnosis (BMI-dx), and three-years post-diagnosis (BMI+3) with lymphoma-specific survival (LSS) as the primary endpoint and with event-free survival (EFS) and overall survival (OS) as secondary endpoints.
Patient and Method: Patients were prospectively enrolled at lymphoma diagnosis to the SPORE Molecular Epidemiology Resource (MER) cohort at Mayo Clinic and University of Iowa from 2002-2015. BMI-2 and BMI+3 were self-reported in patient questionnaires, while BMI-dx was extracted from the medical chart. Patients with extreme BMI (BMI <14 and BMI ≥50) were excluded from the analysis. BMI change from BMI-2 to BMI-dx and from BMI-dx to BMI+3 was categorized as no change (-5% to 5%), decrease (>-5%), and increase (>+5%). Person-time at risk was assessed from lymphoma diagnosis until death or last follow-up, except for analyses of BMI change from BMI-dx to BMI+3, which started person-time at risk when the 3-year (+/- 6 months) follow-up questionnaire was returned. Cause of death was assigned by a study clinician. For all lymphoma patients combined and in the most common subtypes, we evaluated the association of BMI at each time point and change in BMI with EFS, LSS, and OS using hazard ratios (HRs) and 95% confidence intervals (CI) from multivariable adjusted Cox models.
Results: A total of 4,009 lymphoma patients (including 670 diffuse large B-cell lymphoma [DLBCL], 689 follicular lymphoma [FL] and 1018 chronic lymphocytic leukemia/small lymphocytic lymphoma [CLL/SLL] and 1,632 others) with data on BMI-dx were included. Among them, 2,955 patients had BMI-2 and 2,004 had BMI+3 and were evaluable for change in BMI. The median age of all patients at diagnosis was 61 years (range 18-92 years), and 94% of patients had ECOG performance status <2. At the time of diagnosis, 28% were normal weight (BMI 18.5-25), 1% were underweight (BMI <18.5), 39% were overweight (BMI 25-30) and 32% were obese (BMI ≥30). With a median follow-up of 108 months from diagnosis (IQR 83-143 months), 1320 deaths were observed, 48% of which were due to lymphoma.
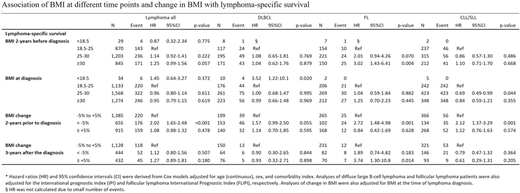
Patients with FL who were obese at BMI-2 had significantly shorter LSS (HR: 3.02, 95%CI: 1.43-6.41, p=0.004). Associations between obesity at BMI-2 and LSS were not evident for DLBCL (HR: 1.04, 95%CI: 0.62-1.76, p=0.879) or CLL/SLL (HR: 1.10, 95%CI: 0.71-1.70, p=0.668) (Table). BMI-dx was not associated with LSS in any lymphoma patients, except that DLBCL patients who were underweight at BMI-dx (n=10) experienced shorter LSS (HR: 3.52, 95%CI: 1.22-10.1, p=0.020). This correlated significantly with presence of B symptoms (p=0.004) and may signify aggressive disease. Across all subtypes, >5% decrease in BMI from BMI-2 to BMI-dx was associated with significantly shorter LSS in patients with (HR: 2.02, 95%CI: 1.65-2.48, p<0.001). However, only for FL patients, >5% increase in BMI from BMI-dx to BMI+3 also was associated with significantly shorter LSS in subsequent years (HR: 3.74, 95%CI: 1.30-10.8, p=0.014). The associations reported for LSS generally were similar for EFS and OS.
Conclusions: FL patients with obesity prior to diagnosis or who experienced increasing BMI after the diagnosis had significantly shorter LSS. The impact of weight control after the diagnosis of FL patient outcomes warrants investigation.
Maurer:Celgene / BMS: Research Funding; Kite: Membership on an entity's Board of Directors or advisory committees; Morphosys: Membership on an entity's Board of Directors or advisory committees; Nanostring: Research Funding; Pfizer: Membership on an entity's Board of Directors or advisory committees. Flowers:Leukemia and Lymphoma Society: Membership on an entity's Board of Directors or advisory committees; Denovo Biopharma: Consultancy; Celgene: Consultancy, Research Funding; BeiGene: Consultancy; Kite: Research Funding; Bayer: Consultancy; Eastern Cooperative Oncology Group: Research Funding; Cancer Prevention and Research Institute of Texas: Research Funding; National Cancer Institute: Research Funding; AbbVie: Consultancy, Research Funding; V Foundation: Research Funding; TG Therapeutics: Research Funding; Burroughs Wellcome Fund: Research Funding; Millennium/Takeda: Consultancy, Research Funding; Acerta: Research Funding; Spectrum: Consultancy; Pharmacyclics/Janssen: Consultancy; Karyopharm: Consultancy; OptumRx: Consultancy; Gilead: Consultancy, Research Funding; Genentech, Inc./F. Hoffmann-La Roche Ltd: Consultancy, Research Funding. Cerhan:NanoString: Research Funding; BMS/Celgene: Research Funding.

